Preoperative surgical planning in three dimensions is a recent but transformative shift in modern medicine. Instead of relying solely on 2D images and intraoperative decisions, surgeons can plan complex procedures in advance, based on an accurate, patient-specific 3D representation of anatomy.
This approach fundamentally changes how surgery is prepared, communicated, and executed.
What is 3D preoperative surgical planning?
3D preoperative planning is a structured process in which the surgeon, together with a multidisciplinary team, prepares the procedure before entering the operating room. Using CT or MRI data, the patient's anatomy is reconstructed into a digital three-dimensional model. The surgeon, radiologist, and medical designer then define:
- Surgical access paths
- Entry angles and trajectories
- Cutting planes and drilling directions
- Implant positioning and fixation strategies
The result is a clear, shared surgical plan tailored to the anatomy of the individual patient.
Why it matters: planning steps in advance reduces uncertainty, improves accuracy, and lets the team focus on execution rather than improvisation.
The role of preoperative simulation
The primary goal of simulation is to let the surgeon prepare as thoroughly as possible. Working with a 3D digital model, or a physical anatomical replica, the team can understand exactly what will be encountered, anticipate technical challenges before they occur, reduce cognitive load in theatre, and communicate more clearly within the team and with the patient.
Simulation turns surgery from a reactive process into a controlled, well-rehearsed intervention.
How preoperative planning is performed
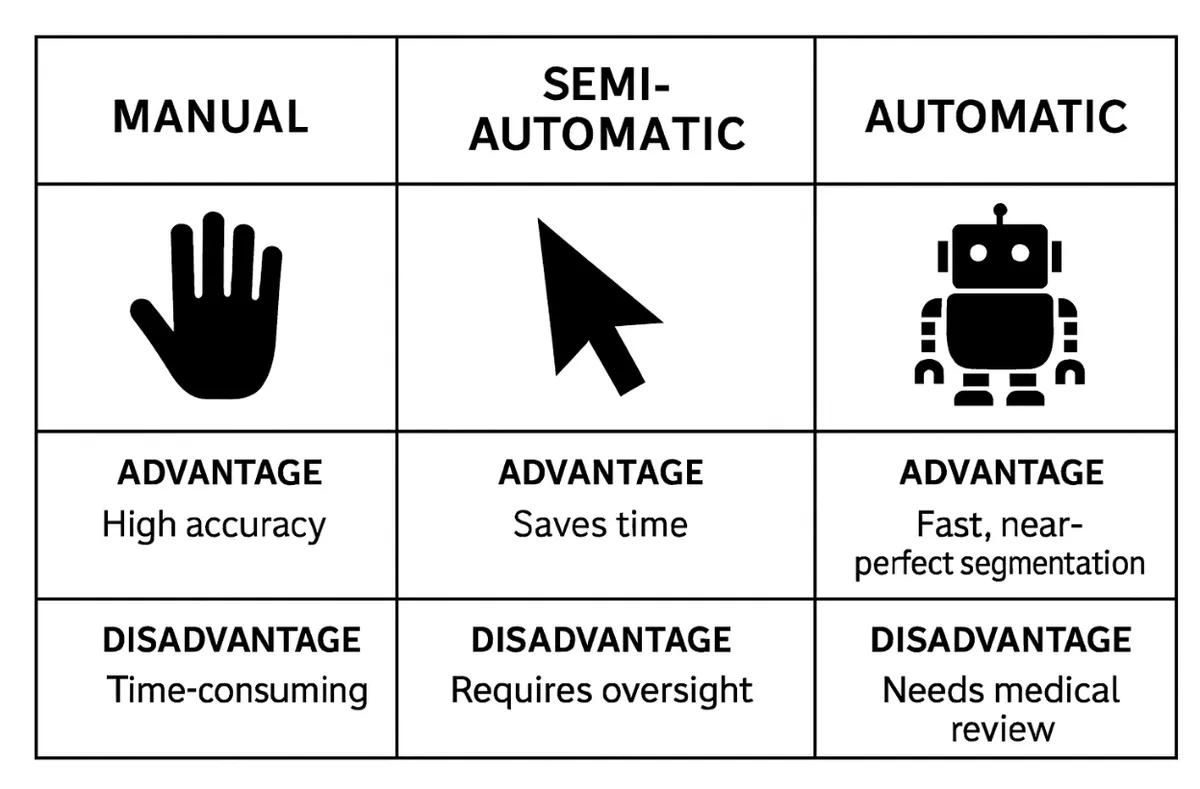
There are two complementary approaches.
1. Digital planning (VR / AR / 3D software)
Using advanced 3D planning tools, the medical designer prepares a digital environment where the surgeon can inspect anatomy from any angle, create cross-sectional views, isolate specific structures, simulate cuts and implant placement, and explore multiple strategies before choosing the optimal one. Virtual and augmented reality further enhance spatial understanding in anatomically complex regions.
2. Physical anatomical models
Patient-specific models can be 3D printed in rigid, flexible, transparent, or tissue-mimicking materials. These let surgeons cut, drill, or saw manually, practice freehand techniques, use patient-specific guides, and test tools and implants physically.
Why physical models matter: hands-on interaction provides tactile feedback and spatial intuition that even the best screens cannot fully replace.
The medical designer: a new clinical role
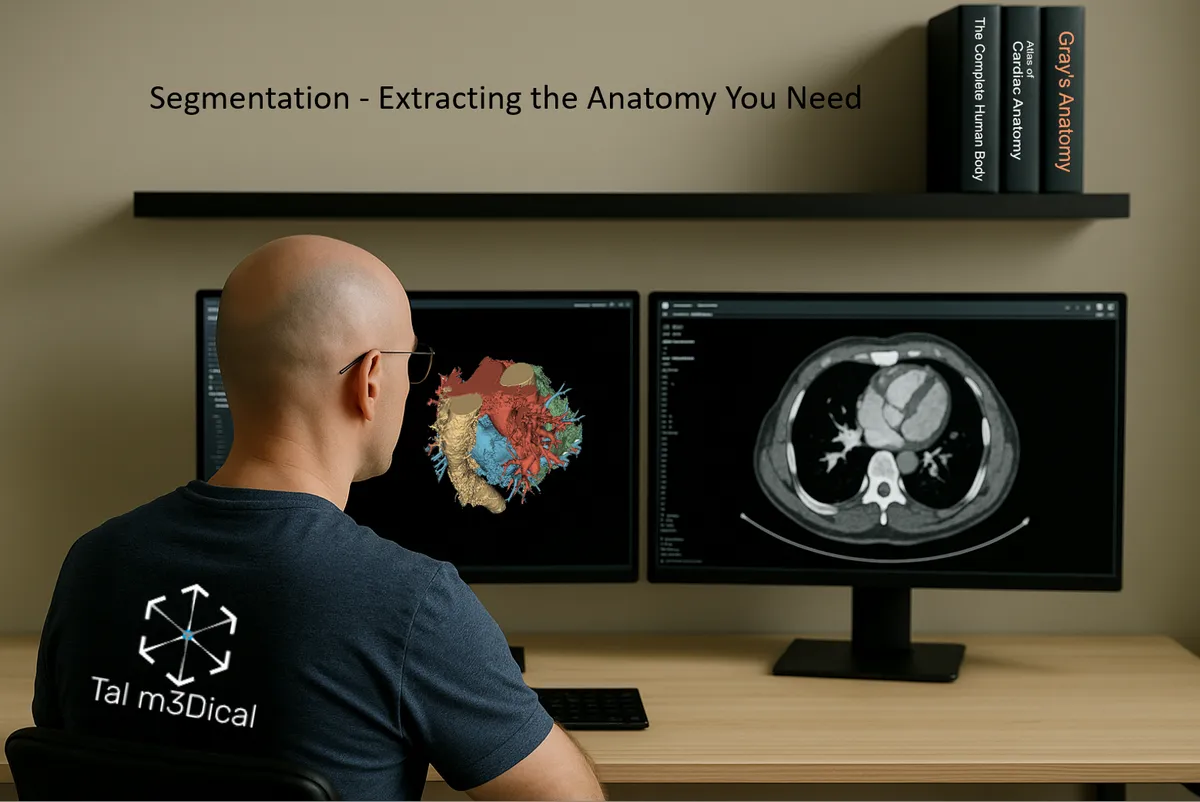
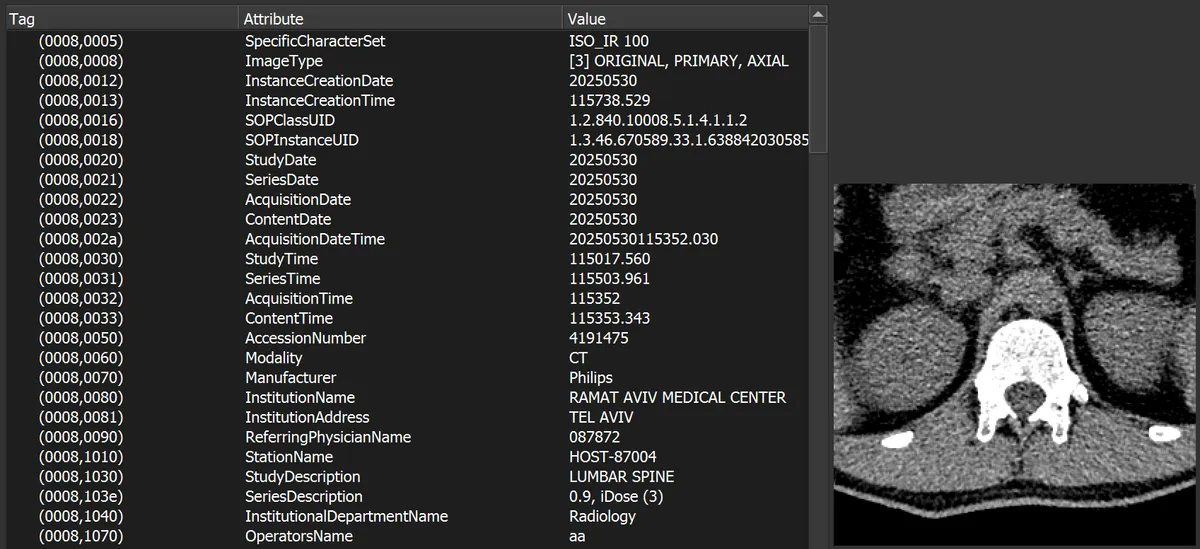
A medical designer is a specialist who bridges medicine, engineering, and digital design. The role requires advanced 3D skills, deep anatomical knowledge, familiarity with surgical workflows, and close collaboration with surgeons. Medical designers perform segmentation, converting 2D imaging data (DICOM from CT or MRI) into accurate 3D models, and then support digital planning, the design of patient-specific instruments, the preparation of anatomical models, and the coordination of 3D printing and post-processing.
Digital surgical planning: step by step
A typical workflow includes:
- Receiving patient CT or MRI DICOM files
- Meeting with the surgeon to define surgical goals
- Clinical analysis: understanding the pathology and objectives
- Defining the surgical approach, tools, and implants
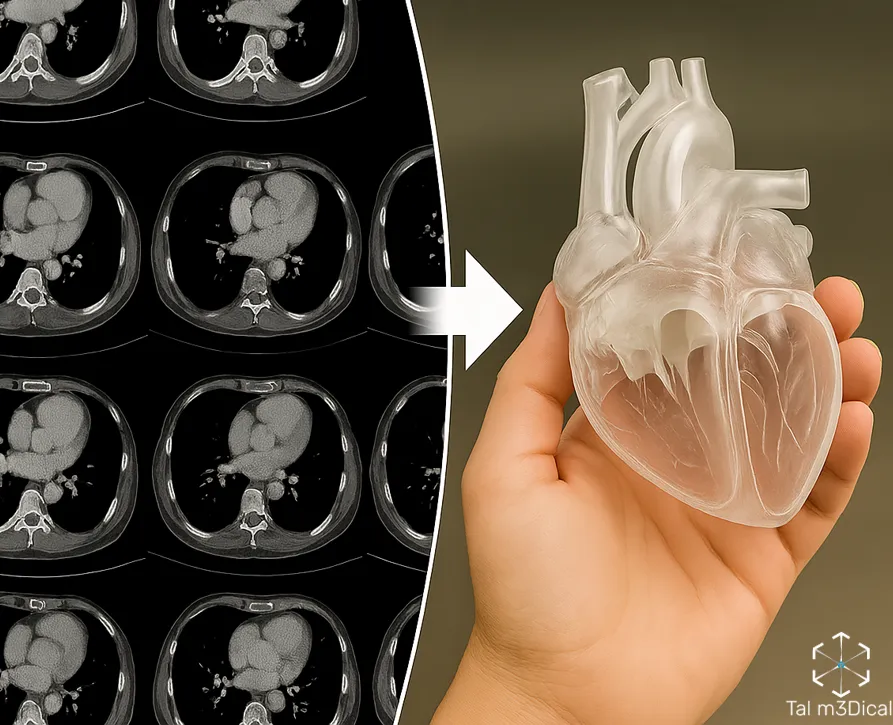
- Segmentation: converting 2D images into a 3D digital model
- Joint surgical planning with the surgeon
- Designing patient-specific instruments (PSI)
- 3D printing of anatomical models and guides
Patient-specific instruments (PSI)
PSI are custom surgical guides designed for a single patient and a single procedure. They may include cutting guides that define exact resection planes, drill guides for precise screw or pin placement, and marking guides for outlining surgical contours. After surgeon approval, these tools are 3D printed in biocompatible materials, cleaned, sterilized, and delivered.
Why PSI matters: it reduces variability, improves precision, and shortens operative time.
Custom implants and reconstruction
In some cases, planning also includes designing custom implants, manufactured from titanium for strength and long-term fixation, or from PEEK, a biocompatible thermoplastic polymer. Custom implants allow reconstruction that follows the patient's anatomy precisely, often replacing generic, off-the-shelf solutions.
Clinical fields using 3D preoperative planning
3D planning and patient-specific tools are used across many disciplines, including orthopedics (deformity correction, fracture reconstruction, scoliosis), orthopedic oncology (tumor resection with bone preservation), hand surgery, maxillofacial surgery, ENT, neurosurgery (cranial reconstruction and rehearsal), cardiothoracic surgery, cardiology, vascular surgery (aneurysms and vascular pathologies), general surgery (liver, kidney, pancreatic tumors), and gynecology and obstetrics.
Common software tools
The pipeline spans three categories of specialized software.
Segmentation
- 3D Slicer
- Materialise Mimics
- 3D Systems D2P
Digital planning and design
- Materialise 3-matic
- Blender
- Autodesk Meshmixer
- Geomagic Freeform
- Rhinoceros 3D
Selecting and combining the right tools for each case is part of the medical designer's craft.
Final thoughts
Preoperative surgical planning in 3D is not just a technological upgrade, it is a shift in mindset. By combining medical imaging, digital design, and physical modeling, surgery becomes more predictable, more precise, and more personalized. The future of surgery is planned, long before the first incision.